What is ICL?
Implantable Collamer Lens (ICL) surgery actually has quite a long history. It was developed in the 1980s, before LASIK (laser in situ keratomileusis) was first reported in 1990. The director general of Sanno Eye Center, Dr. Kimiya Shimizu , was the first doctor in Japan to introduce the ICL procedure in 1997. After clearing a series of clinical trials in 2002, ICL surgery was approved by the Ministry of Health, Labor and Welfare in 2010. However, conventional ICL surgery interfered the circulation of aqueous humor (flow of clear fluid in the eye), and consequently there was a risk of 1~2% of patients developing cataracts.
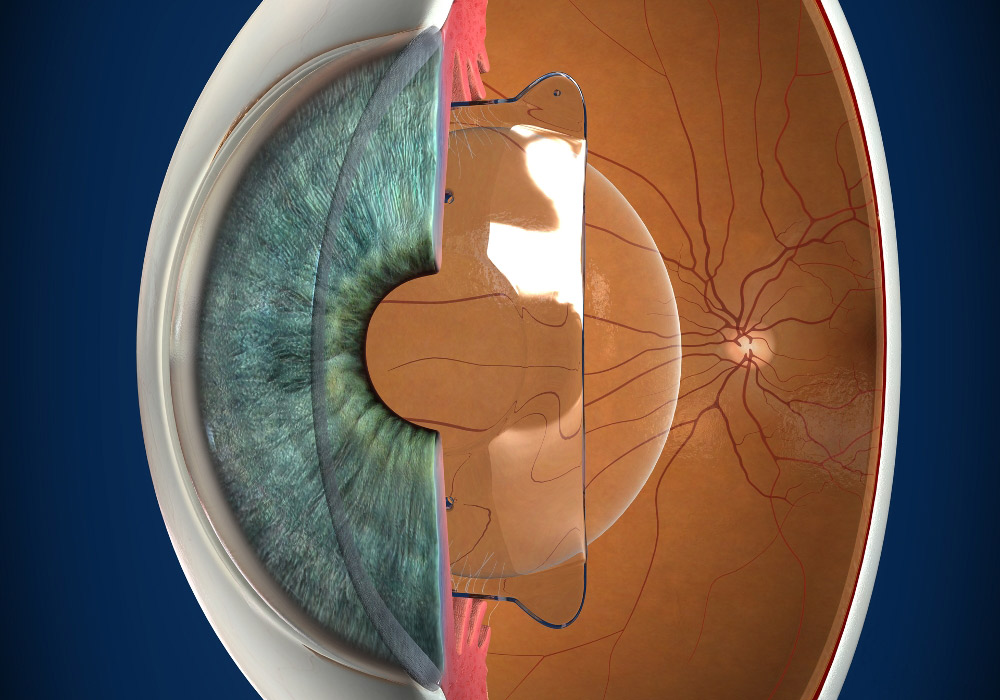
Dr. Shimizu devised and developed the Hole ICL (ICL KS-AquaPORT) surgical procedure of opening up a miniscule hole in the center of the lens to eliminate the complication of cataracts. Then in 2007, he successfully performed the world’s first lens implant. Dr. Shimizu’s Hole ICL surgery improves the circulation of aqueous humor, and subsequently reduces the risks of cataracts developing. It is now approved in over 70 countries around the world as a global standard surgical procedure.
ICL is a reversible procedure; the lens can be easily removed if the patient is experiencing any post-operative discomfort or complications, and the eye is returned to its preoperative state. ICL is also suitable for a wide range of prescriptions. In LASIK surgery, a high level of myopia (near-sightedness) requires a considerable amount of the cornea to be shaved off, which makes the procedure more difficult. Consequently, there is a larger degree of post-operative error and the myopia may reoccur, or the patient could develop dry eyes as a result of the surgery. Also, once the cornea has been shaved it cannot be restored to its preoperative state.
In contrast, ICL surgery uses the same procedure to implant a single lens in the patient’s eye, irrespective of the prescription range; so the surgery has the same level of difficulty for all levels of myopia. Also, even if the patient develops cataracts after ICL surgery, he/she can still be treated with conventional cataract surgery.
Refractive Surgery
Currently, refractive surgery is performed in the following three ways.
-
- Laser surgery to
correct the cornea - PRK, LASIK
- Laser surgery to
-
- Implanting an ICL
in the eye - Implantable Collamer Lens (ICL) surgery
- Implanting an ICL
-
- Replacing the crystalline lens with an artificial lens
- Cataract surgery
Differences with and advantages over LASIK
-
- No post-operative special care required
- Post-operative care only requires regular eye checks, and there is no need for daily maintenance such as washing the lens to keep it clean. The ICL does not become dirty or move around while in the eye.
-
- Wide range of lenses available
- The ICL prescription range covers a high level of myopia (near-sightedness) and hyperopia (far-sightedness), and includes a 6D lens for strong astigmatism (blurred vision). ICL is also suitable for a wider range of prescriptions than LASIK surgery can treat.
-
- No shaving of the cornea
- Once the cornea has been shaved, it cannot be restored to its original thickness. Unlike LASIK surgery, ICL surgery does not require the cornea to be shaved.
-
- Does not cause dry eyes
- The incisional wound is very small at only 3mm, so it does not cause dry eyes, which can result from an abrasion of the trigeminal nerve on the cornea’s surface. (ICL does not improve the symptoms of people who already have dry eyes.)
-
- Day surgery that only takes around 20 minutes
- ICL surgery can be performed on both eyes on the same day in about 20 minutes. It does not require any stitches to be put in or removed, and the incisional wound heals naturally.
-
- Reversible procedure
- The ICL can be taken out if the patient experiences any discomfort, etc.
-
- Performed by certified ICL surgeons
- Unlike LASIK surgery that even non-certified surgeons can do, ICL is performed by a certified surgeon who is specially trained* in the procedure.
*In order to acquire certification, a surgeon must learn the procedures in a certified ICL course, and perform an ICL surgery under the supervision of a certified ICL instructor surgeon.
Post-operative results
Hole ICL surgery (ICL KS-AquaPORT®) performed at the Sanno Eye Center and Kitasato University Hospital between 2007 to 2015 292 eyes of 128 patients available for post-implant follow up
| Gender (Ratio of female patients) |
58.6% (171/292) |
|---|---|
| Age | 34.7 years (between 20 to 54 years) |
| Refraction range | -8.00(+0.50~-23.75D) |
|---|---|
| Astigmatism cylinder | -1.23(0~-7.00D) |
Ratio of uncorrected visual acuity

- This graph shows the ratio of post-operative uncorrected visual acuity. Compared to LASIK surgery, the median uncorrected visual acuity for five years or more after ICL surgery is exceptionally stable at 1.2 and above. This is an excellent result, considering it also includes patients that have always had poor vision and a very high-level of myopia.
Stability: Variation in the refraction range
- 0 indicates normal vision (myopia is completely corrected). Most patients do not experience any post-operative reoccurrence of myopia from the day after surgery and up to seven years later.
Variations in the corneal endothelium cell density
- An ICL is transplanted into the eye, so it is important to ensure there are no post-operative changes in the cells that keep the cornea clear. A healthy person aged in their 20s or 30s normally has around 2,800 to 3,000 of these cells, and this number decreases by several percent with age.
There is no sudden decrease in the number of these cells following ICL surgery, and the cell count remains stable over the long term.
Complications
Early post-operative stage (Directly after to one week later)
| Intraocular pressure rise | 0% |
|---|---|
| Infections | 0% |
Medium to long-term post-operative stage (One week after and up to seven years later)
| Infections | 0% |
|---|---|
| Complicated cataracts | 0% |
| Additional corrective surgery Exchanging the ICL prescription range Astigmatism corrective surgery |
1.4%(4/292) 0.7%(2/292) 0.7%(2/292) |
Between 2007 and 2015, we performed Hole ICL surgery on healthy adults (excluding those with external trauma to the eyes and aged 50 years and over), and none of the patients experienced any infections, rise in intraocular pressure or cataracts.
Only two of the patients (four eyes) required any additional surgery, and one (two eyes) of them switched their ICL prescription range . This patient already had presbyopia (age-related long-sightedness), and initially he wished to alleviate the symptoms while allowing for some level of myopia. He later decided to have ICL surgery, as he wanted to see objects in the distance a little more clearly. So it is also possible to switch the ICL prescription range later on, after the initial surgery.

8-10-16 Akasaka, Minato-ku, Tokyo, 107-0052, JAPAN
- +81(3)-3402-3151 (Main line)+81(3)-3402-3151 (Main line)
- Opening hours: 8:30 a.m. to 5:30 p.m.
(excluding Saturday afternoon, Sunday and Public Holidays)
Please call the Eye Center Outpatient Department
Copyright © Sanno Eye Center. All Rights Reserved.